
NHS Tooth Extractions Are Going Extinct
NHS Dentistry is the the verge of collapse-and the ability to receive tooth extractions or dentures in the system is falling with it. A visualized explanation of the failed state of NHS dental charges. Plus, why NHS dentistry and oral health in England is going back to the past.
We're going back in time....England is in the midst of an oral health crisis not seen since 1945.
Here's the TL;DR:
An outdated, underfunded dental service is letting down both the patients it's supposed to serve...and the dentists who provide the necessary services for citizens.
Which leads to one inarguable fact...
NHS Dentistry is Broken.
And it's difficult to see any sort of momentum to fix the problem.
Dentists are leaving the system. The waitlist for dental care grows by the day. And you are even hearing rumors of...
English Citizens Extracting Their Own Teeth...
...which is not what you would expect to hear from a country with a national health care program. But, the situation has compounded.
COVID finally broke the system, but the foundation has been slowly burning down for the last 16 years.
The Problem Visualized
We're going back to elementary school- because just like your 2nd-grade teacher demonstrated- you can learn something by just looking at pictures.
This visualized article serves as a history book, explanation, and dive into the problems that have weakened the NHS dental system in England.
It's a long, difficult, redundant story.
But it's an important one because NHS dentistry in England is about to hit the point of no return.
Skip Ahead
Who has time to read a 5,000-word article? Not us. So utilize this table of contents accordingly.
👀Buffet Price Dentistry: NHS Dental Charges Explained
🦷A Clinical, Visual Example of UDAs
⏲2007 or 2022? The problems look the same.
👋Dentists are Saying Goodbye and The Treatment Blitz
🎓The Timeline of a Young Dentists
😥Health Inequalities: The Icing on a Fatal Recipe
First, Let's go back to the beginning.
It's the end of World War II and Aneurin Bevan sees a lot of English citizens without teeth.
The Birth of the National Health Service
A Brief History of Aneurin Bevan's Dream, the inception of NHS Dentistry, and Drama Over Dentures
Table of Contents
The second great war had just ended. The Baby Boomers were a sparkle in the eyes of those celebrating a victory on the world stage. And things were changing.
The Labor party had just maintained control of the government and there were some big plans to be made.
Aneurin Bevan, the newly appointed health minister, campaigned to create the form of the NHS that is in place today.
“Health services should be comprehensive, universal and free at the point of delivery"- Aneurin Bevan argued
Like Oprah giving out cars, Bevan said “You get health care, you get health care, you get health care, everyone. gets. free. health. care!” And boy, did he deliver on his promises.
On July 5, 1948 NHS was launched with exactly the core principles he campaigned for...
1️⃣free at the point of delivery
2️⃣It meets the needs of everyone
3️⃣And it’s not based on the ability to pay.
Thankfully, this system started at the perfect time. The oral health of the country was worse than Germany-who was in economic disarray after taking a loss in the war.
The British Needed NHS Dentures
It’s reported that more than 75% of the population over the age of 18 had complete dentures- and more were suffering from dental decay, sepsis, and periodontal disease.
Finally, Bevan Starts the Engine
On July 5th, only about a quarter of practicing dentists were participating in the NHS. But as patients flocked to get their free dental care, the number of dental professionals working in the system exploded.
The patient pool boomed and dentists' schedules were as full as the last clinical day before the New Year.
NHS Dentists Working Overtime
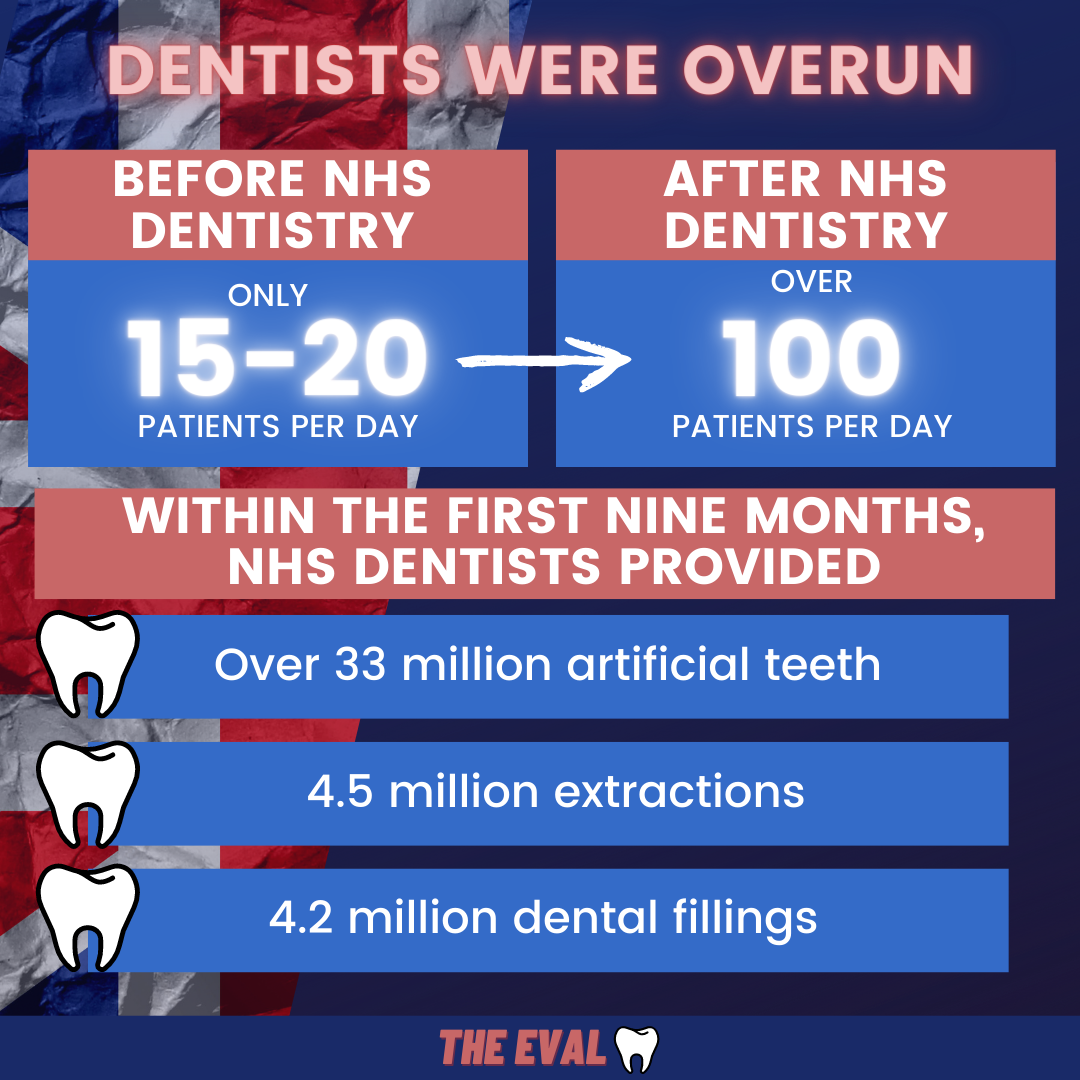
Well that’s what happened, and we can only assume that dentists were drinking some STIFF martinis at the end of their work day. Practices, previously seeing 15 to 20 patients a day, were now seeing over 100.
And the production numbers were staggering. In the first 9 months of NHS existence, dentists performed 4.5 million extractions and 4.2 million restorations (fillings for the non-dentists out there).
Our necks are screaming for a chiropractor just thinking about it.
More Money, More Problems
All was great. The demand for dentistry grew. Oral health of the country improved. Dentists’ incomes rose. And oral professionals flocked to participate in the NHS system.
But, like all great ideas throughout the history of time, this system required one very important thing: money💲💲💲.
Within the first few years, dentists started asking each other at their monthly study club meetings,
"Hey, how’s your practice going. How long do you think this system lasts until the money runs out.” -NHS Dentist, 1951 (probably)
It was a good question. There were real problems (like, how to pay for all of this) and not just hypothetical concerns from dentists at the time (see above).
And so, the government pulls back on the whole, “free dentistry for all, forever" idea and starts charging patients.
The First National Health Service Charges
Trivia Time
At some point in your life, this☝ is going to come up as a question at your local pub’s trivia night. Memorize it now.
If your team would have guessed dentures, you would be correct and you can thank us for your pitcher of beer.
So 1951 hits and the NHS system is just flat out running out of money. The government first decides to start charging for dentures -with more costs not far behind.
The system that Bevan fathered was now no longer what he envisioned. He said, "I don't want to be a part of this", and resigned.
For the next 50 some years, the system (somewhat) maintained. There were always problems and inefficiencies in a large bureaucratic system- but, it survived.
Yet, just 6 years after that whole Y2K scare, things took a turn for the worse.
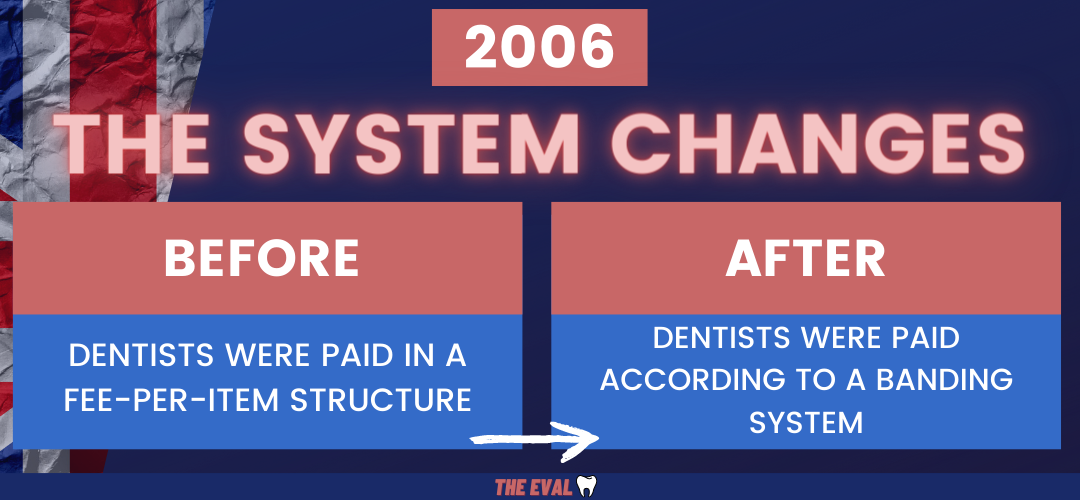
2006: A Bad Inflection Point for NHS Dentistry
A New Contract, the Introduction of Units of Dental Activity, and Buffet-Priced Dentistry
Table of Contents2006: A Bad Turning Point
The year was 2006, the Human Genome Project was completed, Google bought YouTube for (only) 1.65 billion, “Bad Day” was the most popular song of the year, and NHS dentistry took a pivotal turn for the worse.
You could go back through the history of NHS dental services and see multiple instances of failure in the system, but the year 2006 seems to be the inflection point.
Here’s why:
Before 2006, dentists were paid on a “fee-per-item” structure. The more work you did, the more money you earned.
As Ollie Jupes stated in a 2017 Guardian article, “...while many felt that this system was seriously underfunded, it sort-of worked. Treatment was carried out, and dentists were paid for providing it.
But then things changed drastically.
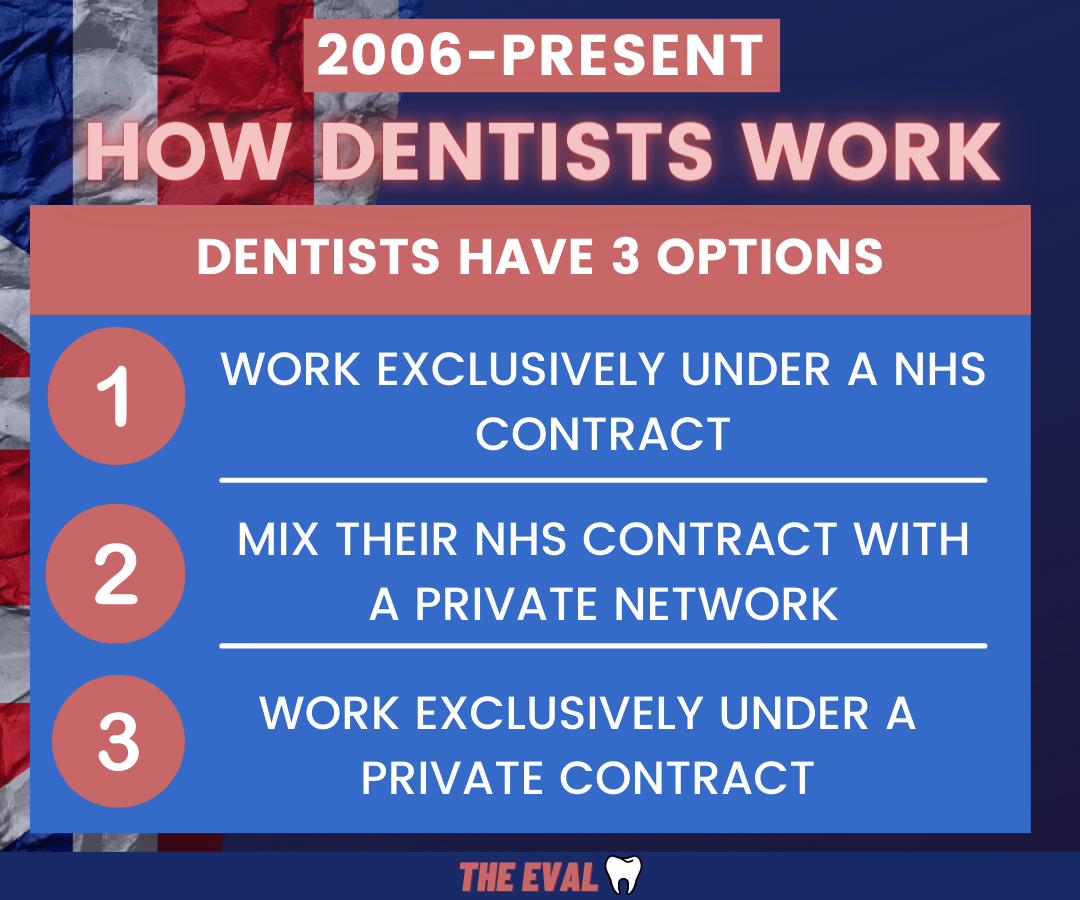
To explain what happened next, we first have to talk about the employment status of the dentists participating in the NHS. British dentists are not government employees, they are private contractors.
Private contractors that are responsible for setting up their own practice, hiring and firing employees, and all their own finances.
They can therefore choose to:
1️⃣Work exclusively under a NHS contract
2️⃣Mix their NHS contract with private work
3️⃣Work exclusively under a private contract
So in 2006, the government changed how they would compensate dentists. This is what happened.
The production of all NHS dentists were analyzed during a "test year" (November 2004 to October 2005). The findings of this research were then extrapolated, calculated and stirred up in a pot to come up with an appropriate contract.
But, fast forward to 2022 and there is a serious problem.
An Outdated Contract
As Dr. Eddie Crouch, the chair of the British Dental Association Board states,
"The average dental earnings from 2004 and 2005 that were used to create this contract are still implemented in the system today."
In no world would dentists use the same outdated materials, techniques, and evidence-based practices today as they did in 2005.
So why is the NHS using the same payment system?
In any case, the government thought this was a good idea for one primary reason: they said that dentists could better predict their budget.
Enter Units of Dental Activity
Also included in this new contract was something that didn't make sense back in 2006...and spoiler alert, it still doesn't make sense today.
UDAs Making Ears Bleed
For some, nails on a chalkboard or the word “moist” can send shivers down the spine. For British dentists, the equivalent phrase is, “units of dental activity.”
Along with the new contract, a new system determining HOW patients paid for their treatment was also implemented. These were some big changes as outlined in this House of Commons Health Committee document.
What did the Health Committee say about the new system:
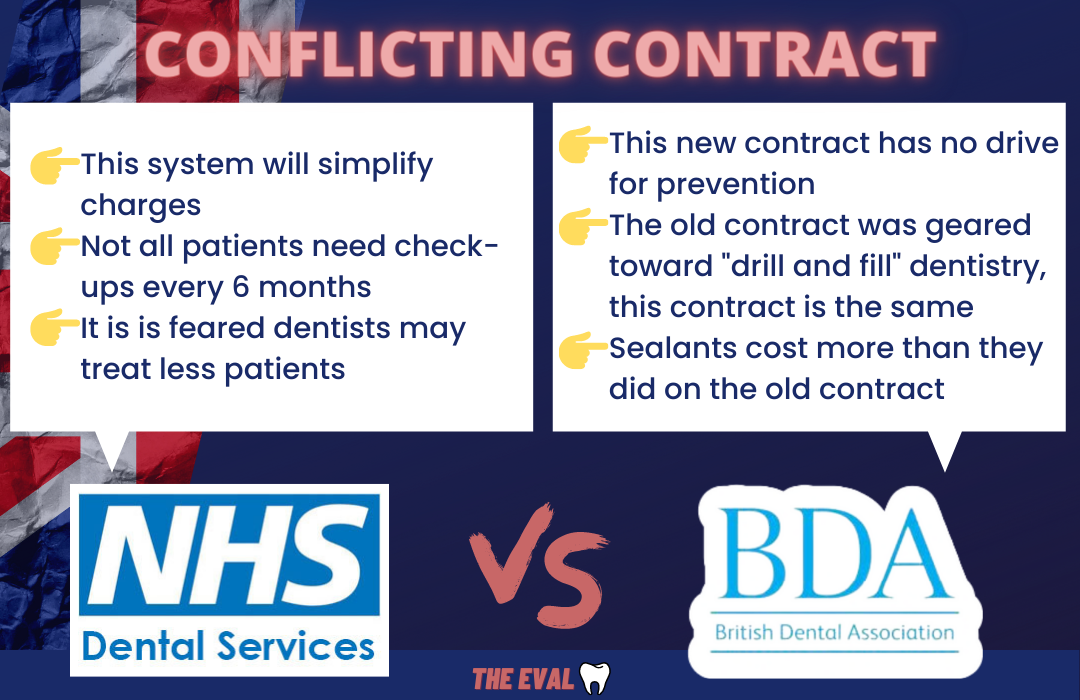
- This new system will simplify charges
- From the advice of the National Institute of Health and Clinical Excellence (NICE), all patients don’t need check-ups every 6 months.
- It is feared that dentists will treat fewer patients because they consider reimbursement inadequate
- Patients won’t try to “store-up” fillings in order to save money.
What did the British Dental Association say about the new system:
- This new contract has no drive for prevention
- The old contract was geared toward “drill and fill” and this new contract is no different
- Preventive care does not attract Units of Dental Activity, therefore dentists won’t feel incentivized to discussed oral hygiene instructions with their patients.
- Sealants cost more now than they did on the old contract
There was also concern that patients will delay their check-ups or store up their dental fillings to save money. The Minister for dentistry, Ms. Rosie Winterton didn’t believe this was the case saying:
I find it very difficult to think that people would say, “If I hang on six months to get another filling, I can get that one in the same band.”… I do think that if people were in that bad a position there would be assistance given through the various schemes.
Overall, government officials didn't listen to the concerns of dentists or the British Dental Association and said, "SEND IT."
Despite all of these conflicting opinions, this new system was a go. And it opened the door to dental practices to become an all-you-can eat dental buffet.
Visualized: NHS Dental Charges
Explaining the system of Buffet Price Dentistry and Units of Dental Activity
Table of ContentsBuffet-Priced Dentistry

When you go to your local Old Country Buffet, you expect that you are going to get a lot of food for a very small price.
To simplify things significantly, this is what the units of dental activity (UDAs) turned into: all-you-can-eat dentistry for one flat price.
NHS Dental Charges: Visually Explained

Here’s how units of dental activity work:
Treatments fall into three different bands: 1, 2, and 3.
- 1️⃣Examinations are band 1 and currently only requires a fee of £23.80 (about 32 dollars). The patients pays about 80% of the cost of treatment which includes an exam, prophy, radiographs, and oral hygiene instruction.
- 2️⃣Band 2 covers filling work, root filling work, extractions, and periodontal treatment. The dentist is compensated roughly £65.20 for this work (about 88 dollars)
- 3️⃣Band 3 includes anything that requires laboratory work including crowns (any number) and dentures. Dentists get compensated £282.90 for this band.
And a few more qualifications according to the National Health Service Website
- If you need another filling within 2 months of the initial diagnosis from the same or lower band- patients won't have to pay anything else out of pocket.
If you take anything from this explanation, it's this simple fact👇.
The NHS Banding system does not properly reimburse dentists. More necessary treatment does not lead to higher financial incentive.

Unless you have really seen the consequences of this system, it’s tough to grasp the significance. So for all the folk out there who prefer not looking in people’s mouth for a living, here’s a real life example that could easily happen in a NHS dental office.
NHS Dental Charges: A Clinical Example
Two patients. Two Different Treatments
Patient 1 (let’s call him Jeremy Jamm) and Patient 2 (let’s call him Tim Whatley) walk into a NHS dental practice.
“It’s been awhile since my last dental visit”
-says both Jeremy and Tim.
Jeremy has some significant problems (too many Sweetums, we reckon). There are multiple teeth that are non-restorable (can’t be saved) and have to be extracted. Other teeth most likely need root canals.
Plus, don't forget about the teeth that need to be replaced. A partial denture is the solution to this toothless problem.
Your Practice has Just Been Jammed
For lack of a more polite description, Jeremy Jamm is a time-suck on your dental practice.
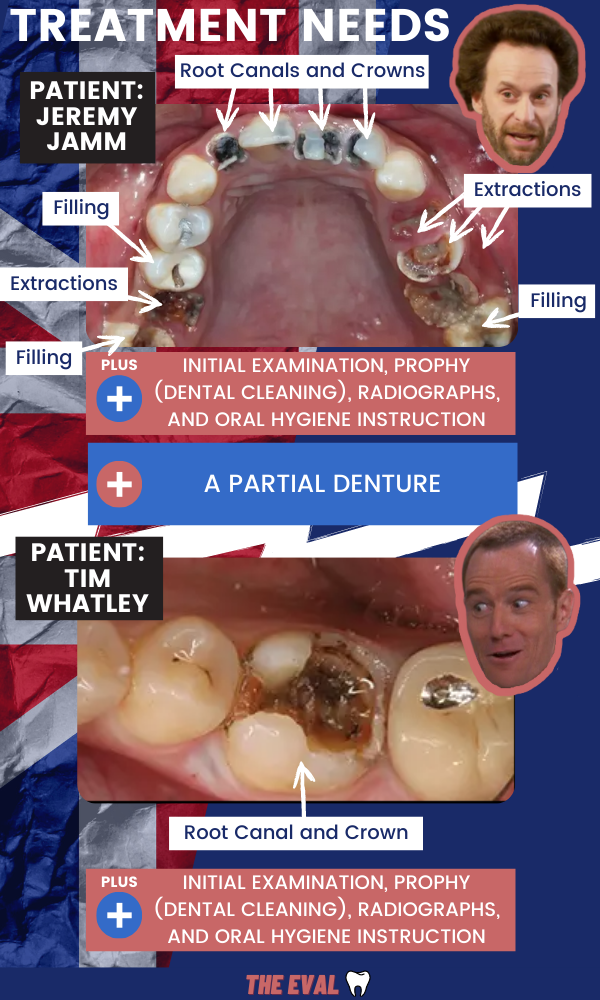
Jeremy needs a lot of dental work which will require a lot of dental appointments. He happily pays only £289.90 for all of the appointments to complete his care .
On the other hand, Tim needs a root canal and a crown in addition to a regular prophy (dental cleaning) and oral hygiene instruction. He pays the same exact amount as Jeremy Jamm despite being able to complete all his treatment in 2 or 3 visits.
But, Tim Isn't Exactly an Easy Patient Either
And just for clarification, even Tim requires a lot of time in the chair for such a low reimbursement fee.
The problem is obvious. Despite very different treatment needs, the reimbursement for payment is just flat out wrong.
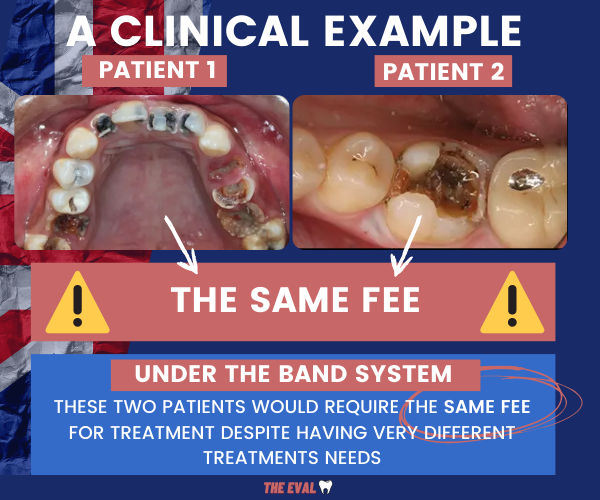
It's Just Not Logical...
From 2006 to 2020, the system acted like a slow leaking dam- always threatening to break but never actually breaking. And the problems with the leak are constant and consistent.
2007 or 2022? The NHS Problems Look the Same.
The idea for a new system was novel. But as we learned from just about every history teacher throughout our education, “history repeats itself.” And dentists were (again) asking the hypothetical but real question over drinks at their monthly study club,
“How are your kids? How is your practice? Do you think dentists can survive in this system?”
And articles from 2007...
Look a lot like the articles in 2022...and 2008 and 2017, for that matter. Same problems, different year.

The BDA Repeating Themselves
If you look at interviews with the leaders of organized dentistry in England, you have to think they get tired of saying the same thing over and over, again.
Peter Ward, the chief executive of the British Dental Association all the way back in 2008 stated,
“They've failed to improve access to care for patients and failed to allow dentists to provide the modern, preventive care they want to deliver....Instead, this contract encourages sporadic, episodic treatment, rather than the long-term, continuing relationships that dentists and their patients value."
Fast forward to today, and Dr. Crouch is saying the same exact thing.
NHS dentistry is at the last chance saloon. For the sake of our patients real, urgent reform cannot remain stuck on the government's 'too difficult' list
The problems with the system are so consistent and confusing it's difficult to keep the years straight.
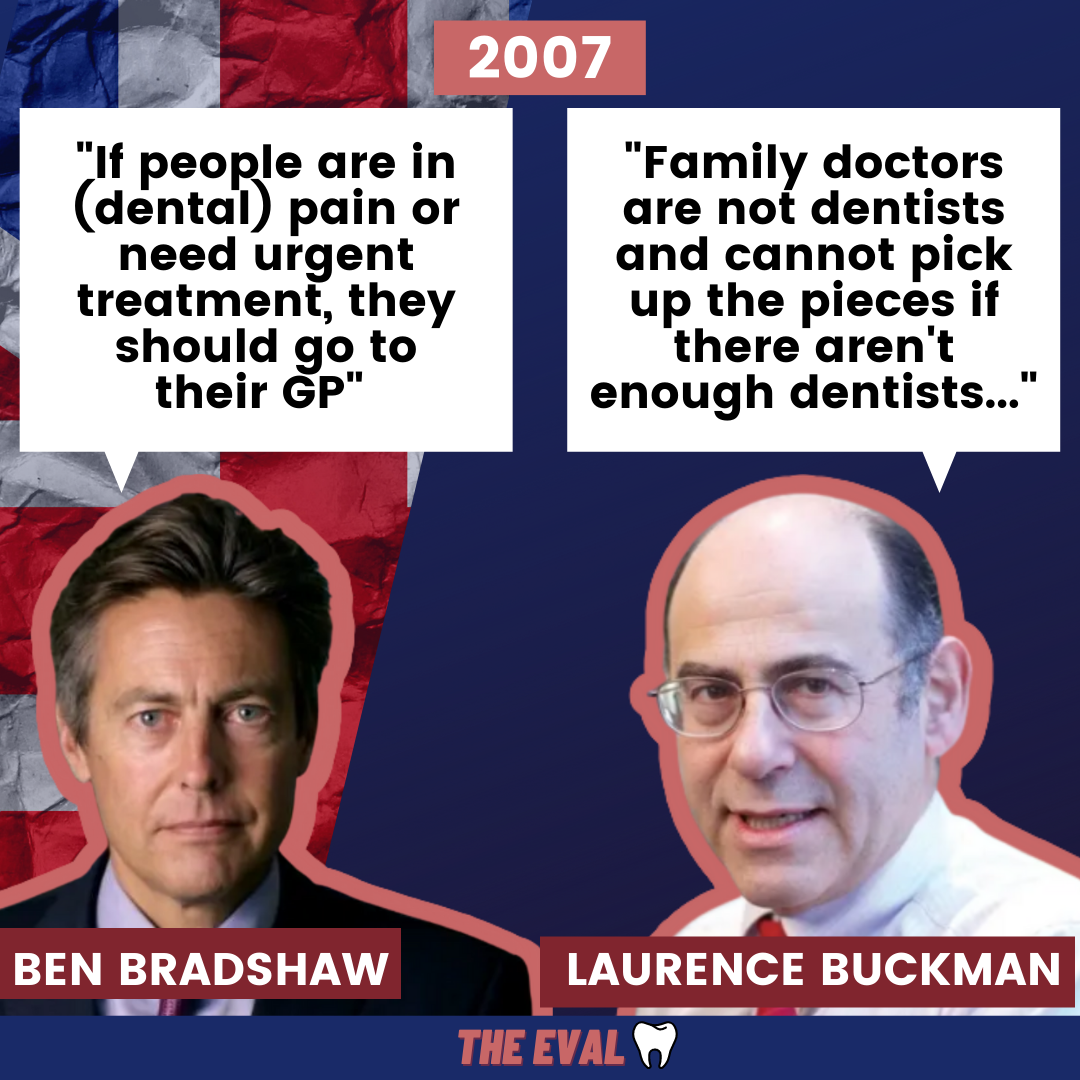
Even leading NHS health officials get confused with the broken system
Which seems very problematic.
The minister of health in 2007 (incorrectly) stated that patients who could not find dental care should turn to their primary care physician for treatment of dental emergencies.
To which, the British Medical Association had to step in and say, “hold up, that’s not correct.”
Disfunction. Disfunction everywhere. How the system survived, I couldn't say.
It's actually a lot like that one long-time, hard-nosed patient of yours...
10 years ago you suggested they get a crown on tooth #30. You are confident they are going to be calling you with a non-restorable fractured tooth in the near future. But somehow, yearly exams come and go with no problems. No crown-it's not nearly as good as it could be- but still maintaining.
Still, it's only a matter of time or one awkward bite of pecan pie on a Saturday night that things go south.
For NHS dentistry in England, that bite of pecan pie came in the form of a history altering event: a global pandemic.
COVID was the Pecan Pie
Right after COVID hit, British dentists were like the rest of us: hanging out at home watching Tiger King, crushing workouts on their Pelotons, and forgetting what day of the week it is.
Offices shut down. 8-10 weeks of no dental work. As a replacement, Crouch says the NHS set up 600 emergency dental care clinics to help with any urgent and emergent treatment patients might need.
As you could guess, this became an odd situation. Would NHS dentists still get paid the contracts they were promised even though they weren’t actively seeing patients?
Yes, but the solution to this problem also included abatement. A 16.75% abatement to be exact. This meant that the NHS would pay the previously agreed upon contracts during lock down- but 16.75% lighter.
As Dave Cottam, GDPC Chair wrote on the BDA blog, the abatement estimated costs of actively running a dental practice including (but not limited to):
👉Laboratory costs and materials (the largest expense at 12.4%)
👉Advertising costs
👉Clinical waste services
👉Travel and subsistence
👉Practice cleaning
Not Perfect. But, Fair.
It wasn't a perfect situation, "...it feels like a fair number" according to Cottam
For those dentists that took on the responsibility of participating as an urgent dental center (UDCs), they were rewarded with no abatement at all.
Dust off the Hand pieces
In June of 2020, dentists could finally get back to work. But it wasn’t exactly opening the flood gates. Many practices struggled with the transition- with the BDA citing cash flow, PPE and child care issues as some of the main culprits of aches and pains.
To cure, these inefficiencies- units of dental activity numbers were tweaked.
First, UDA Targets were Reduced...
...But then ramped up way too quickly.

Reduced, but not reduced enough. After dentists dusted off their handpieces in June 2020, they were expected to hit 40% of their UDA target numbers in order to get 100% of their agreed upon contract.
This 40% goal was soon increased to 85% up until the time of writing.
But it was too much too soon. Only one-third of dental practices were hitting this lofty goal by December of 2021.
And something even more problematic: fallow time
So it was a bit hectic to figure out how to protect yourself when COVID first hit. People were taking horse medication, masks were like an on-again, off-again high school relationship, and dentists in Britain had to adhere to fallow time
If you want an example of a public health measure that had no reasonable evidence-based explanation- look no further than fallow time. This public health measure was instituted after practices re-opened and caused havoc on any productivity dentists were hoping for.
What is Fallow Time?
...waiting one hour after aerosol producing procedures to see another patient in the same treatment room.
In some situations, fallow time is needed. But when high volume suction is used in 94% of dental practices, a full hour break between patients is not supported.
Evidence-based? Negative👎
Ineffiecient? Check✅
But, UDA targets just keep going up
And it continues to pile on. There is indication that the NHS wants dentists to be back at 100% capacity when April 1st hits. A very cruel April Fools indeed.
So what happens should dentists not reach the government’s lofty goals?
A very dreadful word: clawbacks.
As you can imagine, dentists are feeling the pressure. Either become a dental assembly- "drilling and filling" all day everyday to keep up with UDAs.
Or, leave the system.
....and a lot of dentists are choosing the latter.
NHS Dentists Are Saying Goodbye
What do you get when you mix an outdated contract, government clawbacks, and low morale?
Table of Contents...You Get Dentists Going Private.

A new analysis by the BBC showed that NHS dentistry in England and Wales has lost the equivalent of 8% of the workforce. A huge exodus of the system.
Some areas are hit harder than others, many communities around Manchester and Liverpool have lost the greatest percentage of NHS dentists - leading to many stories of patients traveling hours or waiting months for dental care.
But, its just the tip of the iceberg
If you are going to take away anything from this article, I would argue that it's this important fact: things are much worse than they seem.
The data that is making headlines really isn't telling the whole story
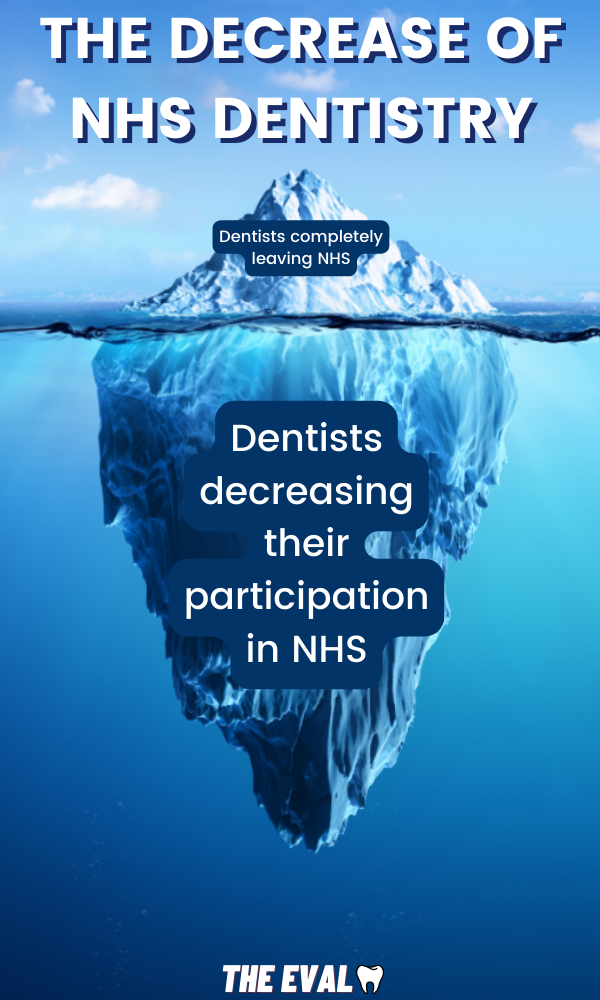
Dr. Crouch makes an important point,
Many NHS dentists have reduced their commitment to the system, but are still on the list of NHS dentists
Here's the Bottom of the Iceberg
In other words, if a dentist has hypothetically decreased their NHS patient load by 95%- they would still show up this list as a practicing NHS dentist.
This leads to a largely misrepresented problem: the situation is much more dire than it looks.
Scrap the System
So dentists are exiting NHS faster than your employees leave on Friday afternoon. What's the logical solution?
Complete overhaul of course. Burn the current UDA system down to the ground. Get a new contract. Implement a system that patients and dentists deserve.
But no, not the plan.
Instead, the decision was made to put some Flex Tape on a leaky hole.
Enter the Treatment Blitz
When there are thousands of patients on a waiting list to receive dental care, it’s not surprising that some short-term fix needs to be done. So what was the solution?
💥The Treatment Blitz: a 50 million pound influx of money being sent to NHS dentists to work evenings and weekends in order to decrease the waiting list.
Recycled Money
No one will complain when additional funds are sent to an already severely underfunded system. But remember those Toy Story-esq clawbacks that took place when dentists failed to hit the inflated UDA numbers post-COVID?
It seems illogical to take money away in the form of clawbacks only to give it back a few months later
It's almost like the money is just being recycled back into the system.
Politicians Gonna Politic
At best- this is a very poor attempt to fix the problem.
At worst- this is just a political play to win over voters so government officials can say, “hey look, we are trying to fix the problem.”
It's estimated that it would take 880 million pounds of funding to restore the system back to it's 2010 levels.
Again, patches and politics over total fixes.
So is this Treatment Blitz going to help at all?
Dr. Crouch says no,
It won't be successful...what will happen is that the local NHS will take [too much] time to distribute the money and the dentists won't have much time [to take care of the backlogs]

The Timeline of a Young NHS Dentist
Plus, why health inequalities are the topping on a very bad recipe for disaster.
Table of ContentsWhen young recently graduated dentists get out of school, they are eager and ready to serve patients. And I would wholeheartedly argue that the majority want to put their education to use in order to serve those that truly need help.
Private dentist jobs are rare without previous experience. So most new graduates enter the NHS.
But, they quickly realize that the NHS dental system doesn’t simply allow for you to just dip your toes in the water, its a dive head first into a riptide.
As Dr. Maha, a 2018 graduate of the dental school at King’s College in London, describes,
All of a sudden, the one-and-a-half-hour treatment planning sessions in dental school have been dramatically shortened to fifteen-minute back to back checkups and emergencies.
It's a stressful existence for new graduates- still trying to hone their skills while simultaneously being thrown into a treadmill of work environment.
A Stressful Timeline
A typical timeline of a young dentist after their graduation from 5 years of dental school includes:
🎓"Safe Beginners". You can't learn everything in school. Graduates are competent, but they will need to learn more to keep up with the fast-demand of private practice. Which is why a Dental Foundation year exists.
1️⃣A Dental Foundation Year. A year to get some experience under you belt. For many young dentists in the NHS system, this may feel like trial by fire.
🥼Mentorship...under a general dentist "trainer" who is experienced in the NHS system.
As. Dr. Maha says,
For me, this year brought more value than most of my undergraduate years; learning how to practice dentistry in an environment, where materials and equipment are not as freely available as they were in dental school.
Please Don't Leave
Young dentists are a valuable resource in the NHS. Eager, hard-working, and fresh with with the latest knowledge...they will serve their patients diligently.
But, how long will these young dentists stick around? At some point, working in a treadmill of a practice with very small financial incentive starts to hurt. Both mentally and physically.
According to Dr. Crouch, fresh-faced NHS dentists get payed only about thirty-thousand pounds per year- with the average NHS dentist bumping up to sixty-five thousand pounds.
Life Continues On
Growing families. Student loan payments. Mortgages. And a stressful work environment with minimized financial incentives....
Many will go private seeking greener pastures.
A Public Health Recipe for Disaster.
One last important thing to help put into perspective of why NHS reform is so direly needed: health inequalities.
“Pay for your own dental care! If you can’t find a NHS dentist just pay out of pocket. Simple solution!”
Long waits have become more and more prevalent in the NHS dentistry system. But for patients that are financially able to pay out of pocket for dental care, there are options...find a dentist and go private.
As more dentists leave the system, fee-for service dentistry will become more and more common.
But long waits and less providers leads to a very concerning...
...Recipe for Disaster
Health inequalities are a big problem in dentistry. This is hammered into dentists' brains during school, but often overlooked in the real world.
A very recent, and very topical Danish study showed the impact of irregular dental care and low socioeconomic status on tooth loss.
- Adults with irregular dental visits are 2.4 times more likely to have fewer than 15 teeth.
- Low-income adults were 5 times more likely to have fewer thann 15 teeth.
And a Very Gross Result
Combine a massive wait list, NHS dentists leaving the system, and a system that doesn’t put any precedence on oral health prevention- you are going to have a lot of people with fewer than those 15 teeth. And it’s not going to be the ones that can afford dental care out of pocket.
Whatever Happens, It Needs to Happen Fast
Right now, it looks bleak. The system has been a problem since the start with no changes along the way. Maybe, just maybe COVID has given the ill-positioned snowball enough of a push to actually cause change.
A reform is already being tested to the west. According to Couch and the BDA, Wales is piloting a new system that will hopefully address some of the issues that the current UDA contract experiences.
The proposed argument from all the way back in 2006 still holds true. Prevention drives the system. And thankfully it could be coming.
Here’s how it works:
- Every patient is risk assessed to help establish their schedule for dental care. Patients are classified into red, amber, and green risk levels.
- This risk assessment is determine by things such as home care, high sugar and soda intact, and other diet habits.
- With this risk assessment, not all patients are recalled at the same intervall. The patients that need more care and attention, receive more care attention.
But for now, hop in the Delorean...
We're Going Back to the Past.

With every passing day of fewer dentists and fewer appointments, comes a backlog of patients that will soon turn into an even more urgent public health crisis.
From April 2020 to December 2021, 40 million less courses of treatment were administered. 40 million.
And the time machine is about to hit 88 miles per hour.
History is repeating itself.
Back to 1945 we go. Back to the public health crisis. Infection, sepsis, dental infections, and dentures galore.
Maybe change is coming. But for now, things are going to get much worse before they get better.